23/01/2009
Aphasia is a complex communication disorder that can significantly impact an individual's ability to express themselves and understand others. It arises from damage to specific areas of the brain responsible for language processing. While there are various forms of aphasia, this article will delve into non-fluent aphasia, a condition characterised by difficulties in producing speech.

- What is Aphasia?
- Symptoms of Aphasia
- Types of Aphasia
- Causes of Aphasia
- Stages of Aphasia Recovery
- Risk Factors
- Duration of Aphasia
- Is Aphasia Contagious?
- When to Seek Medical Help
- Potential Complications
- Diagnosis and Assessment
- Treatment for Aphasia
- Preventing Aphasia
- Rehabilitation Strategies
- Aphasia vs. Alzheimer's Disease
- Key Terminology
- Bilingualism and Aphasia
- Assessing Aphasia
- Mechanisms of Language Recovery
- Therapeutic Approaches
- Frequently Asked Questions
What is Aphasia?
As defined by Dr. Bertrand Glize, a rehabilitation physician specialising in this pathology, aphasia is an oral and/or written language disorder resulting from a brain lesion affecting language centres. This can lead to a partial or total loss of communication abilities, potentially accompanied by other impairments such as difficulties with writing or reading. Aphasia can be profoundly debilitating, affecting a person's family, social, and professional life.
In France, the National Federation of Aphasics estimates that around 300,000 people are affected by aphasia. The severity and manifestation of associated symptoms can vary greatly among individuals.
Symptoms of Aphasia
On a daily basis, individuals with aphasia struggle with speaking, understanding, reading, or writing. There are several forms of aphasia, each with distinct characteristics:
Language Production Difficulties (Non-Fluent Aphasia)
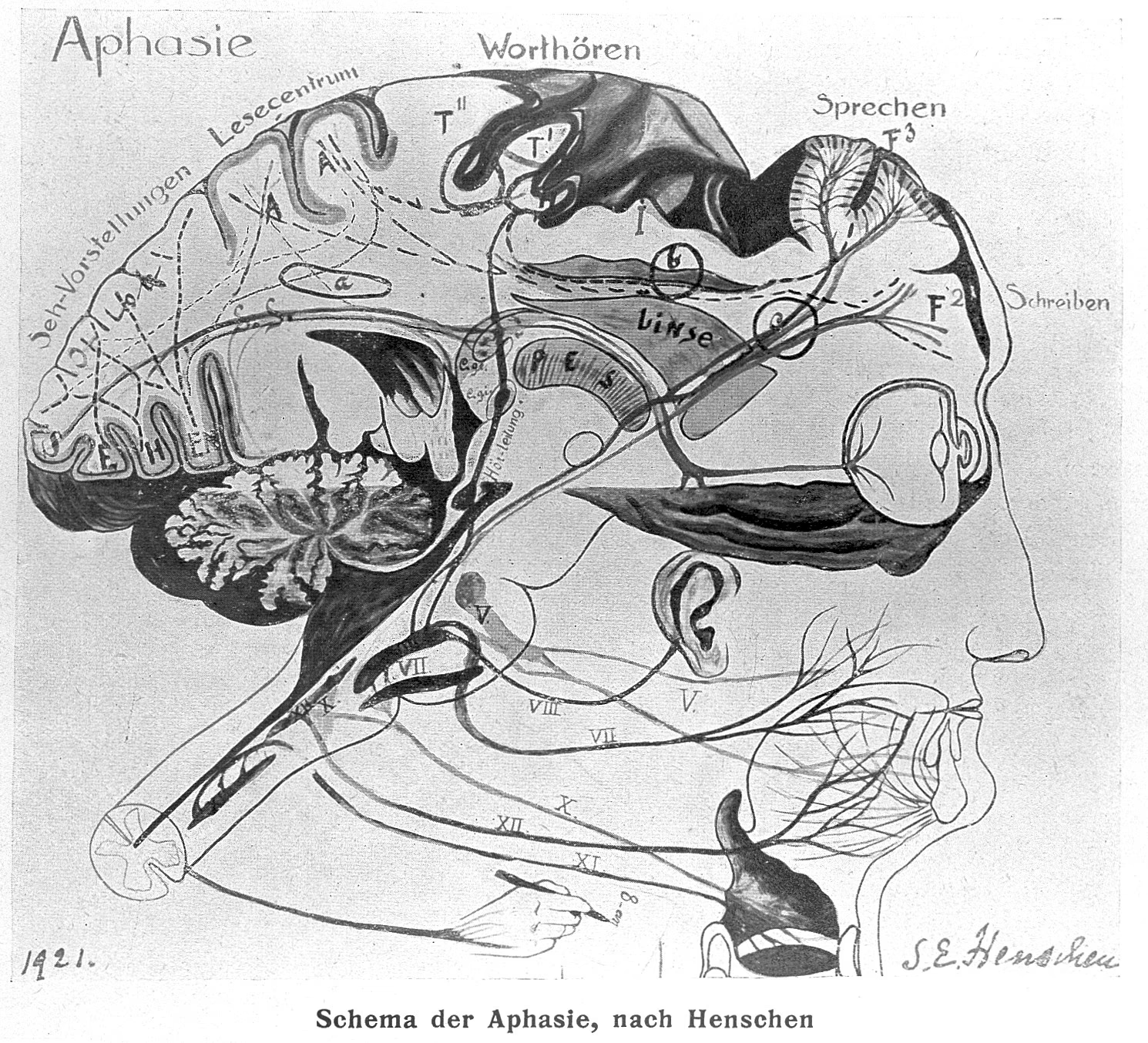
This category encompasses difficulties in producing words correctly, often accompanied by a reduction in verbal fluency – the speed and flow of speech. This is the hallmark of non-fluent aphasia. The spectrum of these impairments ranges from the common 'tip-of-the-tongue' phenomenon (anomia), where individuals struggle to retrieve specific words, to more severe production deficits. Historically, Broca's aphasia, described by Paul Broca, is a classic example of non-fluent aphasia, primarily affecting language production with relatively preserved comprehension.
Language Comprehension Difficulties
In contrast, Wernicke's aphasia, described by Karl Wernicke, is characterised by significant comprehension deficits. While speech fluency may be maintained, the individual's output can be filled with jargon and nonsensical phrases, as they lack the ability to critically assess and understand their own speech.

These symptoms can manifest in both spoken and written language, not always in equal measure.
Types of Aphasia
Beyond the well-known Broca's and Wernicke's aphasias, specialists have identified other forms based on the varying proportions of comprehension and production impairments:
- Conduction Aphasia: Characterised by fluent speech, but often interrupted by hesitations and paraphasias (word substitutions). Comprehension is generally good.
- Global Aphasia: Involves severe impairments in both language production and comprehension. Speech output is minimal, and understanding is significantly affected.
- Primary Progressive Aphasia (PPA): A neurodegenerative condition that causes a gradual decline in language abilities over time. It can sometimes be an early symptom of diseases like Alzheimer's.
Causes of Aphasia
The term 'aphasia' originates from the Greek words 'a' (without) and 'phasis' (speech), meaning 'absence of speech'. It is a symptom of brain damage stemming from various causes, including:
- Stroke (Cerebrovascular Accident - CVA): This is the most common cause, with an estimated 20-30% of stroke survivors developing aphasia.
- Head Trauma: Injuries to the brain from accidents or impacts.
- Brain Infections: Such as encephalitis.
- Brain Tumours: Abnormal growths within the brain.
- Neurodegenerative Diseases: Including PPA, which can be linked to conditions like Alzheimer's disease.
Stages of Aphasia Recovery
Following a stroke, aphasia typically progresses through three phases:
- Acute Phase: In the immediate aftermath of the brain injury, the brain undergoes significant changes. Patients often require intensive care. Initial symptoms can be severe, including complete mutism. Rehabilitation efforts begin during this phase.
- Subacute Phase: The brain starts to reorganise itself, with affected but undamaged areas reactivating. Intensive speech therapy is crucial during this period, as it's when the most significant progress is often seen. This phase can also be emotionally challenging as the individual becomes more aware of their cognitive changes, potentially leading to depression.
- Chronic Phase: Neuroplasticity mechanisms become less intense. While progress continues, it is typically more gradual. The condition becomes integrated into the individual's daily life.
Risk Factors
While aphasia can affect anyone with brain damage, older adults are more commonly affected. Age is a contributing factor to strokes, tumours, and neurodegenerative diseases. However, age is not the sole determinant; brain injury at any age can lead to aphasia.
Duration of Aphasia
The extent of recovery varies greatly from person to person and depends on several factors:
- Cause, Size, and Location of the Lesion: The nature of the brain damage plays a crucial role.
- Type and Severity of Aphasia: Different forms and severities of aphasia have different recovery trajectories.
- Associated Disorders: The presence of other conditions can influence recovery.
- Treatment and Response: The effectiveness of therapy and the individual's response to it are vital.
Is Aphasia Contagious?
No, aphasia is a symptom of brain damage, not a contagious disease.
When to Seek Medical Help
Sudden difficulties in speaking should be treated as a medical emergency, potentially indicating a stroke. Immediate medical attention (calling emergency services) is crucial to restore blood flow, save brain tissue, and improve the chances of recovery. Every minute counts.
Potential Complications
Brain lesions causing aphasia can lead to secondary complications such as memory impairment, difficulties with organisation, or motor deficits. It's common for aphasia to co-occur with hemiplegia (paralysis on one side of the body) due to the proximity of language centres to motor control areas in the brain.
Diagnosis and Assessment
Diagnosing aphasia typically involves:
- Clinical Examination: To assess speech difficulties and rule out other conditions like dysarthria (speech articulation problems), hearing loss, or vision problems.
- Brain Imaging (MRI): To determine the extent, severity, and cause of the brain lesion.
- Further Tests: Additional assessments may be conducted based on the suspected cause.
Treatment for Aphasia
Treatment for aphasia is tailored to the underlying cause. If aphasia is due to a brain tumour, treatment for the tumour is prioritised. The cornerstone of aphasia treatment is speech and language therapy (SLT). SLT aims to help patients improve their language functions and enhance their quality of life. Intensive therapy, with multiple sessions per week, is often recommended, especially during the subacute phase. Patients are also encouraged to practice exercises at home. Alternative communication methods, such as gestures and drawing, can also be valuable tools.
Preventing Aphasia
Since aphasia is a symptom, prevention focuses on preventing its underlying causes, particularly strokes. Key preventative measures include:
- Maintaining a healthy, balanced diet.
- Quitting smoking.
- Limiting alcohol consumption.
- Engaging in regular physical activity.
- Managing high blood pressure.
Rehabilitation Strategies
Speech and language therapists, in collaboration with other healthcare professionals and the patient's family, lead aphasia rehabilitation. The goal is to improve communication. It's important to note that the degree and duration of recovery cannot be predicted precisely.
Aphasia vs. Alzheimer's Disease
While both conditions affect cognitive functions, there are distinctions. Alzheimer's disease is often characterised by a higher frequency of absent or indeterminate responses compared to aphasia. Conversely, specific formal approaches in language assessment are more commonly observed in aphasia than in Alzheimer's.
Key Terminology
Anomia (Word-Finding Difficulty)
Individuals with anomia struggle to retrieve specific words, much like having a word on the "tip of their tongue." They might resort to synonyms or descriptions. This isn't a memory issue per se, but a difficulty in accessing the correct word at the right time. The word may reappear later in a different context.
Paraphasias
These are errors in word production. Verbal paraphasias involve substituting a word with another (e.g., saying "glasses" instead of "spectacles"), while phonemic paraphasias involve substituting or transposing sounds within a word (e.g., "culvitateur" for "cultivateur").
Jargon Aphasia
In jargon aphasia, the speech is so distorted with incorrect words, sound substitutions, or neologisms (made-up words) that it becomes unintelligible.
Stereotypy
Some individuals with aphasia may produce the same word or syllable repeatedly, regardless of the context (e.g., "My God, my God" or "ta, ta, ta").
Comprehension Difficulties
This involves trouble understanding spoken or written language, with comprehension of short sentences or isolated words varying among individuals.
Bilingualism and Aphasia
Bilingual or multilingual individuals with aphasia typically experience impairments in all languages spoken. Research suggests that while often both languages are affected similarly, there can be instances of alternating antagonism between languages or differential recovery patterns. Tests like the Bilingual Aphasia Test (BAT) are designed to assess aphasia across multiple languages, accounting for cultural and linguistic nuances.
Assessing Aphasia
Various tests, such as the Bordeaux Verbal Communication Scale and the Lille Communication Test (TLC), are used in France to evaluate the degree of aphasia. These assessments help identify specific language deficits, including difficulties with writing, reading, conversation, and financial tasks.
Mechanisms of Language Recovery
Recovery from aphasia, primarily driven by the brain's neuroplasticity, involves several mechanisms:
- Reactivation of the Damaged Area: Restoring blood flow and neural connections within the injured region.
- Activation of the Left Hemisphere: The dominant hemisphere for language plays a crucial role.
- Compensation by the Right Hemisphere: The non-dominant hemisphere may attempt to take over language functions, though this can sometimes be associated with less optimal recovery.
Functional MRI (fMRI) can help identify which recovery mechanism is at play, guiding therapeutic interventions. However, practical limitations like cost and accessibility can make fMRI challenging for widespread use.
Therapeutic Approaches
Since damaged neurons are not replaced, recovery hinges on forming new neural connections. Speech therapy is paramount. Methods like music therapy, which leverages the right hemisphere's processing of melody and rhythm, can be beneficial, particularly for accessing automated speech patterns.
Frequently Asked Questions
What is the difference between dysphasia and aphasia?
Aphasia is an acquired language disorder resulting from brain damage in individuals who previously had normal language skills. Dysphasia, while sometimes used interchangeably, can also refer to developmental language disorders present from childhood, or sometimes to a less severe form of aphasia. The key distinction lies in the acquired nature of aphasia following a brain injury.
What is the difference between aphasic and Alzheimer's?
Aphasia is a language disorder caused by specific brain lesions, whereas Alzheimer's is a progressive neurodegenerative disease that affects multiple cognitive functions, including memory, thinking, and language. While language difficulties are present in both, the underlying pathology and the range of affected cognitive domains differ.
If you want to read more articles similar to Understanding Non-Fluent Aphasia, you can visit the Automotive category.